

March 2024
Variable QRS morphology during a physiological pacing implant
Lloyd Tudor, Specialist Cardiac Physiologist, Leeds Teaching Hospitals NHS Trust
Disclosure: The author has no conflict of interests to declare.
Background
During a physiological pacing (Left Bundle Branch Area Pacing) implant, a dual chamber pacemaker was inserted with an atrial lead in the right atrial appendage and a ventricular lead in the right ventricular septum with the intention of capturing the cardiac conduction system.
A ventricular threshold test was performed and it was noted that the morphology of the paced QRS complex changed during the test prior to a loss of ventricular capture. The test was conducted in VVI mode, decrementing from an output of 5.0 V. The change in QRS morphology occurred at an output of 2.5 V remaining this way until capture was lost at 0.5 V. The QRS duration also changed from 122 ms to 109 ms at this time.
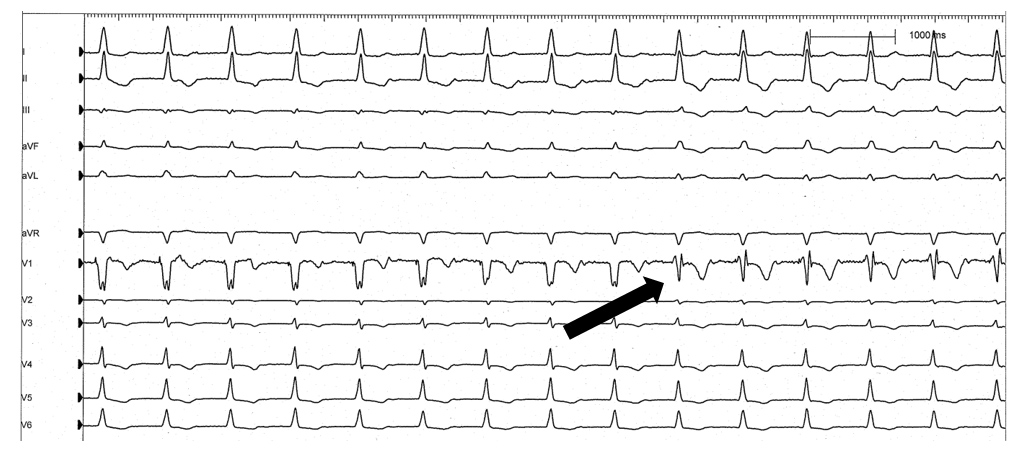
Figure 1. ECG of the ventricular threshold test with the paced QRS morphology change highlighted.
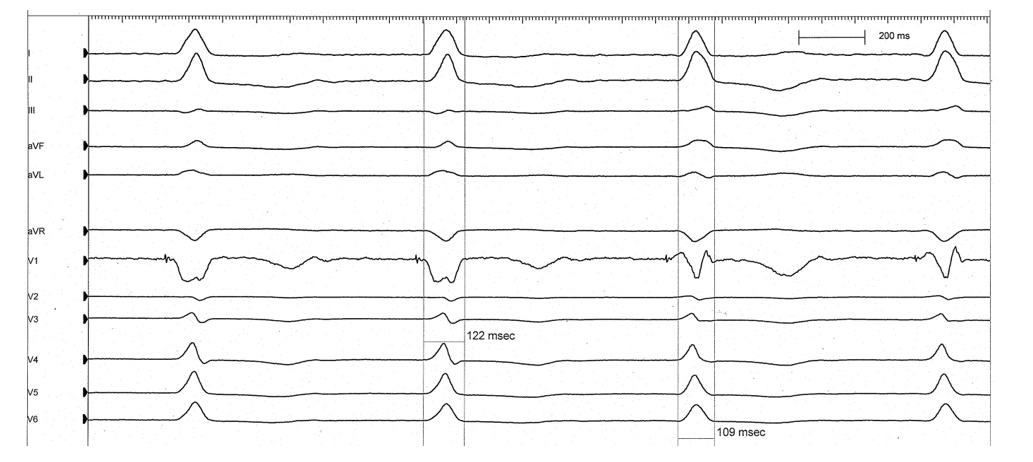
Figure 2. ECG of the QRS morphology change at a sweep speed of 100 mm/s
QUESTION
What does the change in morphology seen in figure 2 represent?
Disclaimer: The British Heart Rhythm Society (BHRS) collates submissions for the ECG/EGM challenge on this website. These submissions, along with any accompanying answers, are provided by external contributors and are published for informational purposes only. BHRS does not endorse, guarantee, or warrant the accuracy, completeness, or reliability of any submissions or answers provided.