

November 2021
Post Box Change EGM Interpretation
Hayley Langridge
Lead Cardiac Physiologist, St Georges University Hospitals NHS Foundation Trust
Disclosure: The author has no conflict of interests to declare.
Background
An 86 year old female attended the device clinic for her 6 week post box change pacemaker check. On device interrogation, 310 AT/AF electrograms (EGMs) had been recorded. Figure 1 is representable of all available EGMs on the device.
Programmed device settings are displayed below.
Mode: AAI – DDD
Max Track: 120 bpm
Mode Switch: 171 bpm
RA sensitivity: 0.9 mV
Sensed AV Delay: 200 ms
Lower Rate: 60 bpm
Max Sensor: 120 bpm
PVARP: 250 ms
RV sensitivity: 2.8 mV
Paced AV Delay: 230 ms
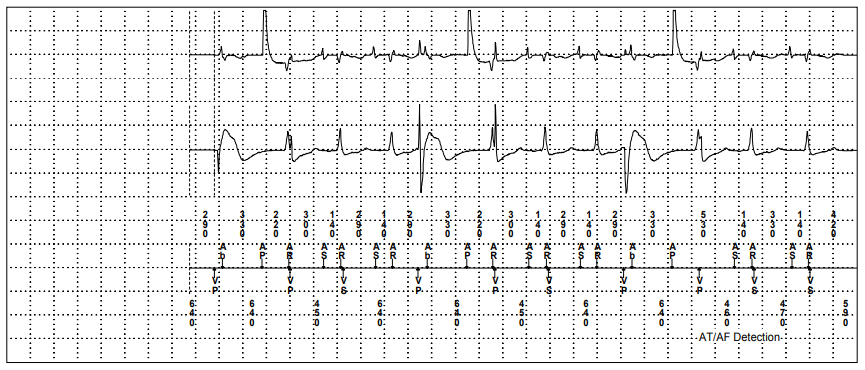
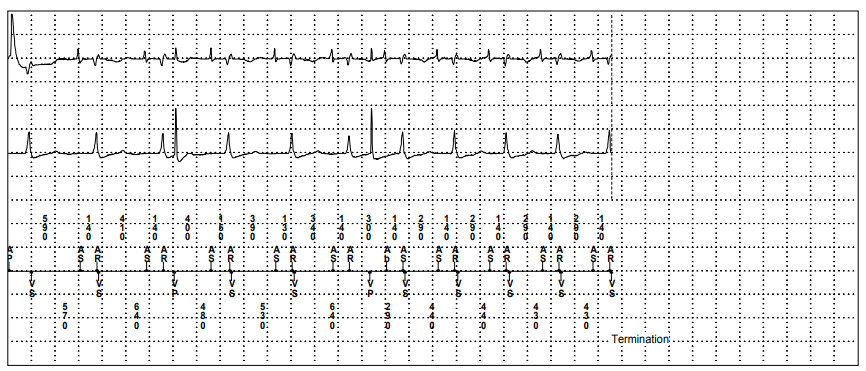
Figure 1: AT/AF stored EGM. Channel 1: Atrial Bipolar EGM, Channel 2: Ventricular Bipolar EGM, Channel 3: Device Markers.
QUESTION 1
What is the cause of this episode?
Answer
Far field R wave
Explanation
The EGM displays more atrial events than ventricular events. After or on time with each ventricular event there is a deflection recorded on the atrial channel marked predominantly with an AR (atrial refractory) marker. These deflections are typical of far field R wave oversensing.
The device is programmed to mode switch to prevent the tracking of fast atrial arrhythmias and records an EGM when the atrial rate is faster than the programmed mode switch rate. In this instance the mode switch rate is set to 171 bpm (350 ms). Figure 2 shows that the criteria for AT/AF detection has been met as all atrial intervals shown within the red box are < 350ms along with there being consistently more atrial events than ventricular events.
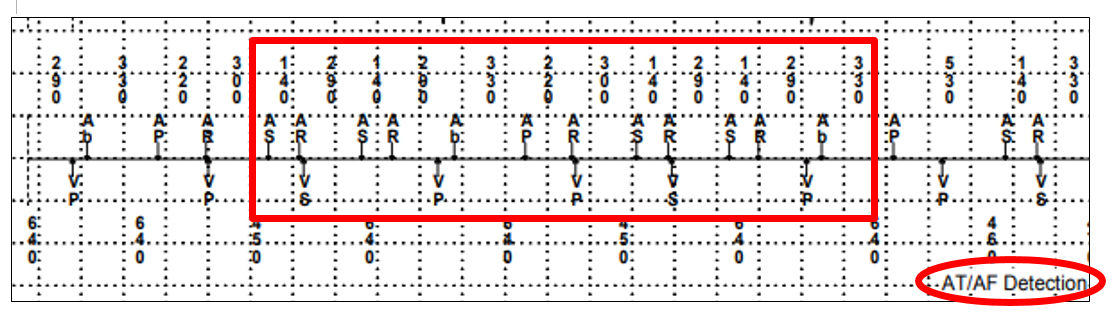
Figure 2: EGM Marker. Channel 1: Device Markers.
QUESTION 2
What is the most important programming change to make for this patient?
Answer
Increase ventricular sensitivity
Explanation
To reduce far field R wave oversensing on the atrial channel the best programming change would be to decrease the atrial sensitivity which would make it less likely to sense the far field R wave. However, this change is not the most important change to make. Figure 3 is a zoomed in section of the EGM in figure 1. Seen in the red boxes there is clear R wave undersensing with inappropriate ventricular pacing being delivered in the ventricular repolarisation period (T wave) which is known to be pro-arrhythmic and has a risk of initiating ventricular arrhythmias.
In the red boxes, the device atrially senses (AS) an atrial event. There is a deflection on the RV EGM 140 ms later which is an intrinisic R wave, this beat is undersensed as no (VS) marker is recorded. The next atrial event is a sensed far field R wave which falls in the atrial refractory period marked as an AR. As the device ventricularly undersensed the AV interval was not reset and times out at the programmed interval, 200ms. At this point the device initates a ventricular paced (VP) event and in these two examples this ventricular paced event coincides with the replorisation period. Consequently, the most important programming change required from this trace is to increase the ventricular sensitivity.
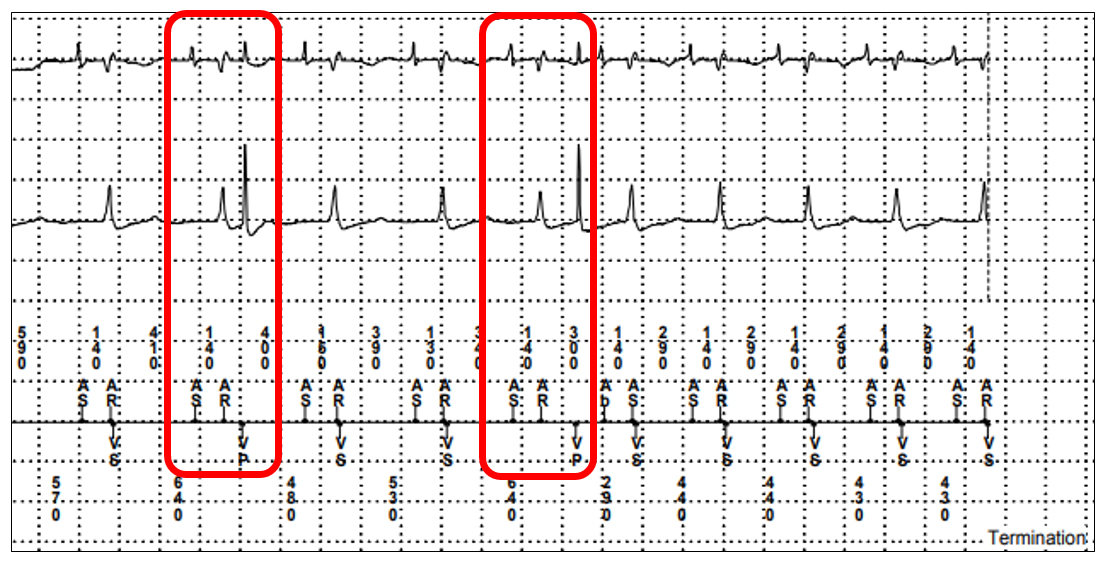
Figure 3: Ventricular Undersensing EGM. Channel 1: Atrial Bipolar EGM, Channel 2: Ventricular Bipolar EGM, Channel 3: Device Markers.
In Conclusion
In conclusion, this case highlights how it is important to review all data present in recorded EGMs when assessing for potential device malfunctions. Careful assessment of each lead, channel and the associated markers was key to identifying the two lead issues seen here. Where issues are identifed in one lead it is essential that the function of the other lead is not overlooked.