

September 2019
Bradycardia on Telemetry following a pacemaker implant
Jason Collinson – Chief Cardiac Physiologist
Essex Cardiothoracic Centre, Basildon and Thurrock University Hospital
jason.collinson@btuh.nhs.uk
A 60 year old male was implanted with a Sorin/MicroPort dual chamber pacemaker following an emergent admission for syncope associated with intermittent AV block. Three hours post implant telemetry captured an episode of bradycardia displayed in figure 1. An urgent pacemaker check was requested with concern that there was device malfunction. The device settings programmed at implant are displayed below.
Mode: AAI-DDD (SafeR)
Lowere rate: 60 bpm
Upper rate: 130 bpm
Paced AV delay: 220 ms
Sensed AV delay 155 ms
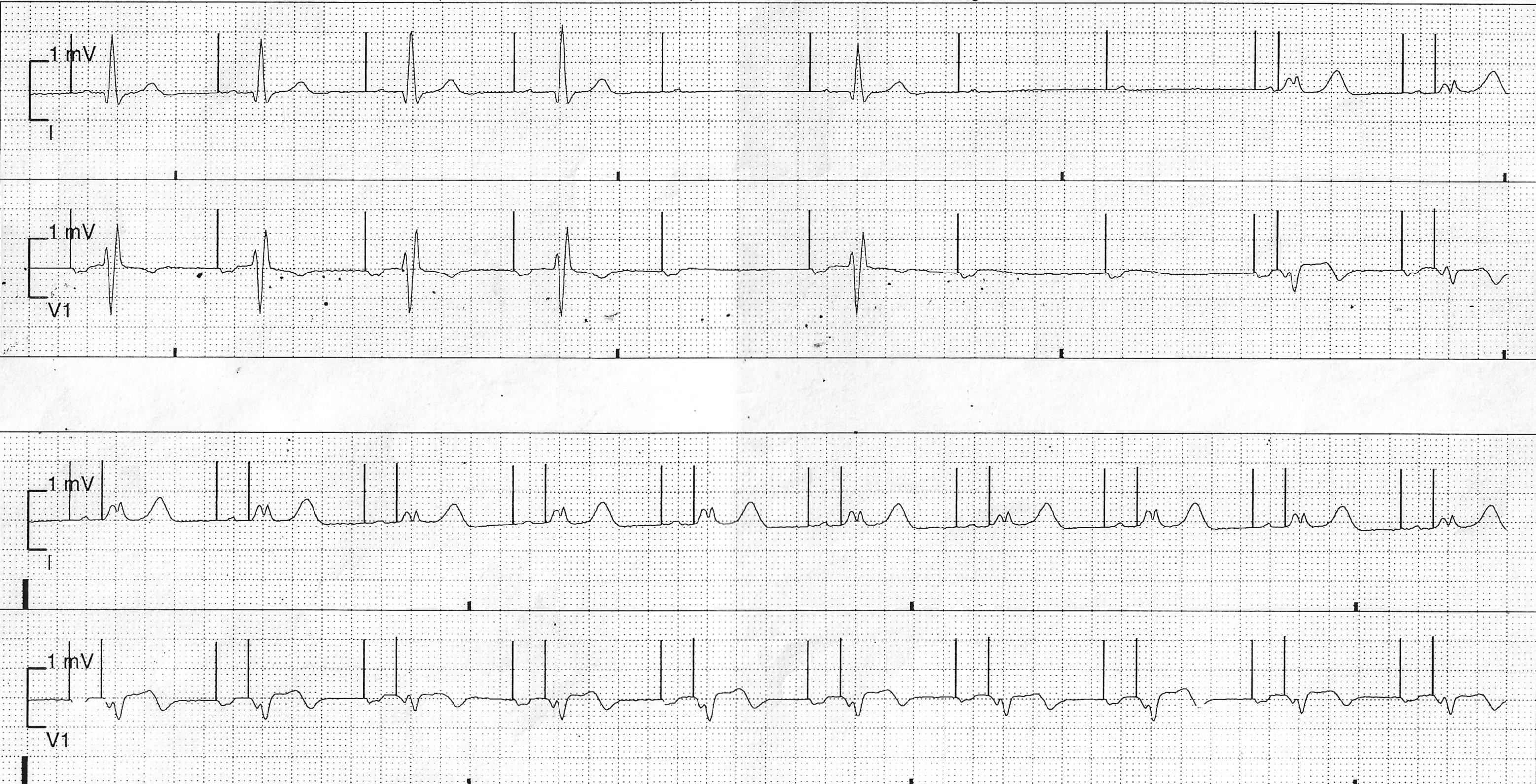
Figure 1
Telemetry recording showing an episode of bradycardia a few hours after de-novo pacemaker implant. ECG leads displayed are lead I (top) and V1 (bottom)
QUESTION
Which answer best explains the telemetry recording?
Answer
Normal pacemaker behaviour
Explanation
The telemetry recording displays normal pacemaker behaviour for the programmed settings and shows a mode switch episode from AAI pacing to DDD pacing caused by an episode of AV block.
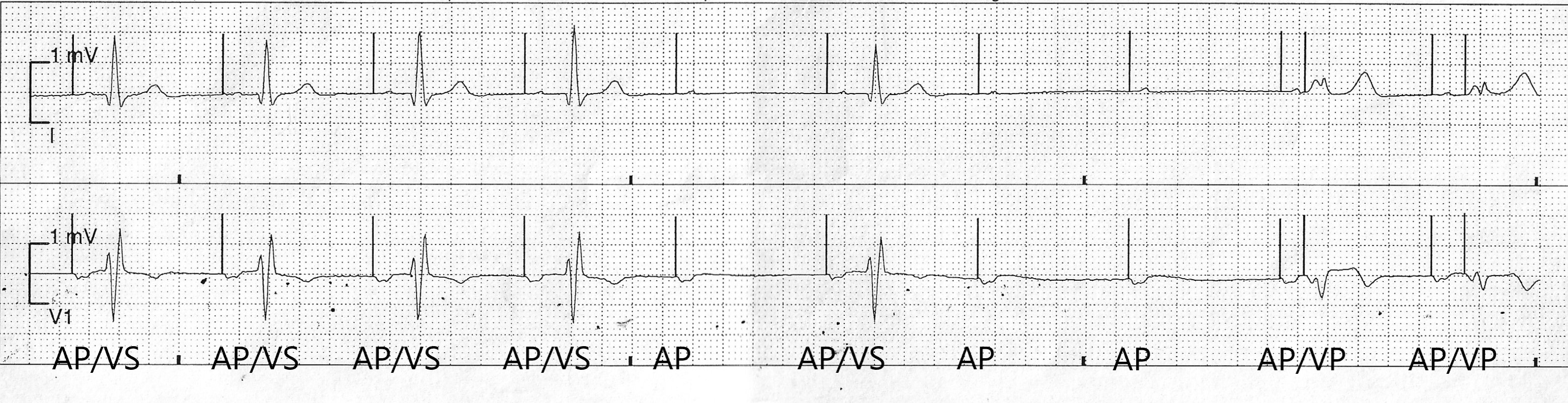
In the trace we can see the first four atrial paced (AP) beats conduct to the ventricle giving rise to an intrinsic QRS complex with right bundle branch block (rSR pattern in lead V1). There is subtle prolongation of the AV interval with each consecutive AP event. The 5th AP beat captures the atrium but fails to conduct to the ventricle. The 6th AP beat conducts to the ventricle. The 7th and 8th AP beat both fail to conduct to the ventricle and this triggers a mode switch from AAI to DDD pacing. The rest of the strip shows atrial paced (AP) and ventricular paced (VP) beats. (Note. there is a clear change in QRS morphology with ventricular pacing)
The trace is an ECG example of Sorin/MicroPort’s SafeR algorithm in operation.
SafeR is one of several manufacturer specific algorithms designed to reduce unnecessary ventricular pacing which can help reduce the detrimental effects of RV pacing in patients with sick sinus syndrome and intermittent AV block.
The algorithm works by providing AAI pacing (this is actually ADI pacing with the ability to sense events in the atrium and ventricle) whilst monitoring AV conduction. If loss of AV conduction is detected by any of the four specific criteria below the pacing mode switches from ADI pacing to DDD pacing restoring AV synchrony.
The 4 criteria used to detect loss of AV conduction are;
- AVB I Criteria – 6 consecutive long PR intervals
- AVB II Criteria – 3 non conducted atrial events out of 12 consecutive cycles
- AVB III Criteria – 2 consecutive blocked atrial events
- Pause Criteria – V-V interval greater than the programmed pause duration (programmable at 2 or 3 seconds)
In this example there were 2 consecutive blocked atrial events therefore mode switch was triggered after AVB III criteria was met.
For this case a device check confirmed normal pacemaker function consistent with the programmed settings. Stored SafeR EGM’s confirmed an appropriate mode switch to DDD pacing with AVB III criteria met. The patient was asymptomatic to the episode however the SafeR settings were reviewed and a minor change made to the pause criteria brought in to 2 seconds from the nominal 3 seconds. Through making this minor change the length of bradycardic episodes is reduced when a pause or 2 blocked atrial events occur forcing mode switch to DDD pacing to occur quicker and reducing the potential risk of bradycardia induced symptoms.