

April 2024
Recorded Pause On ICM
Matthew Carson Chief Cardiac Physiologist, Aberdeen Royal Infirmary
Disclosure: The author has no conflict of interests to declare.
Background
A patient had an Implantable Loop Recorder implanted due to a background of two syncopal episodes. The day after implant the following recording was received.
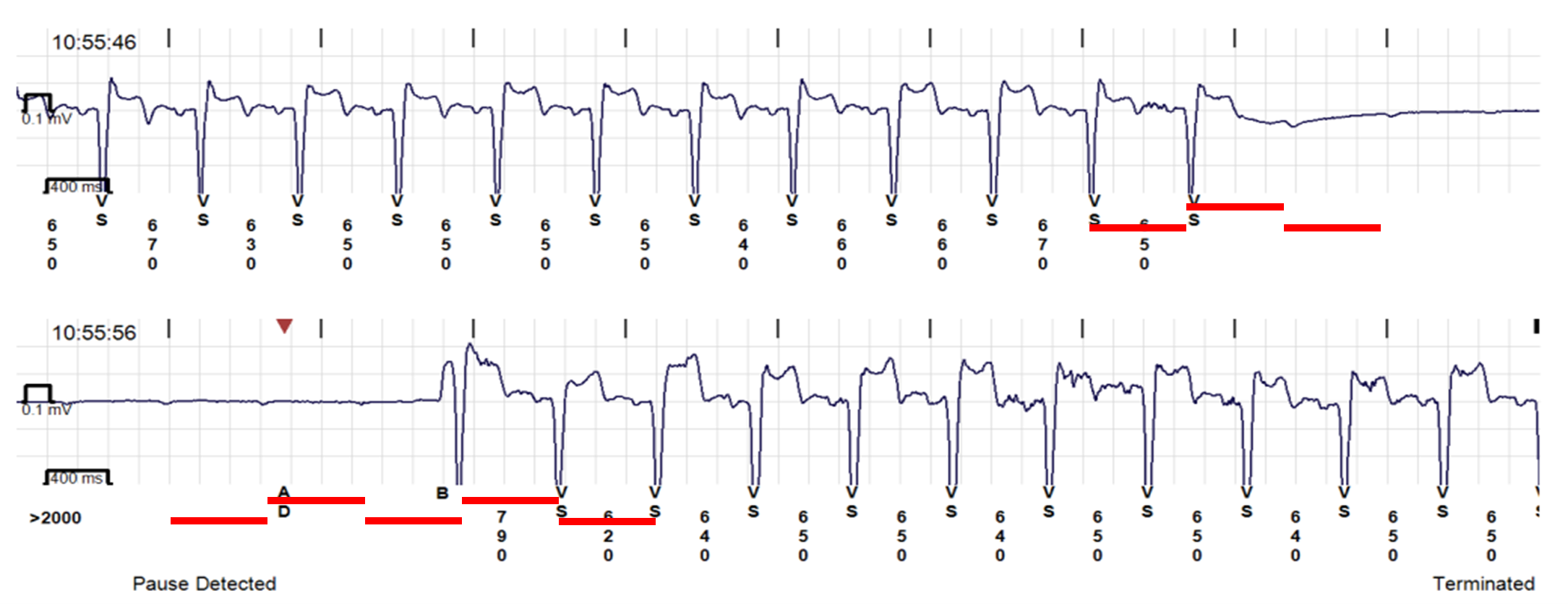
Figure 1
QUESTION
What is your diagnosis?
Answer
Normal sinus rhythm with under-sensing of QRS complex
Explanation/Discussion
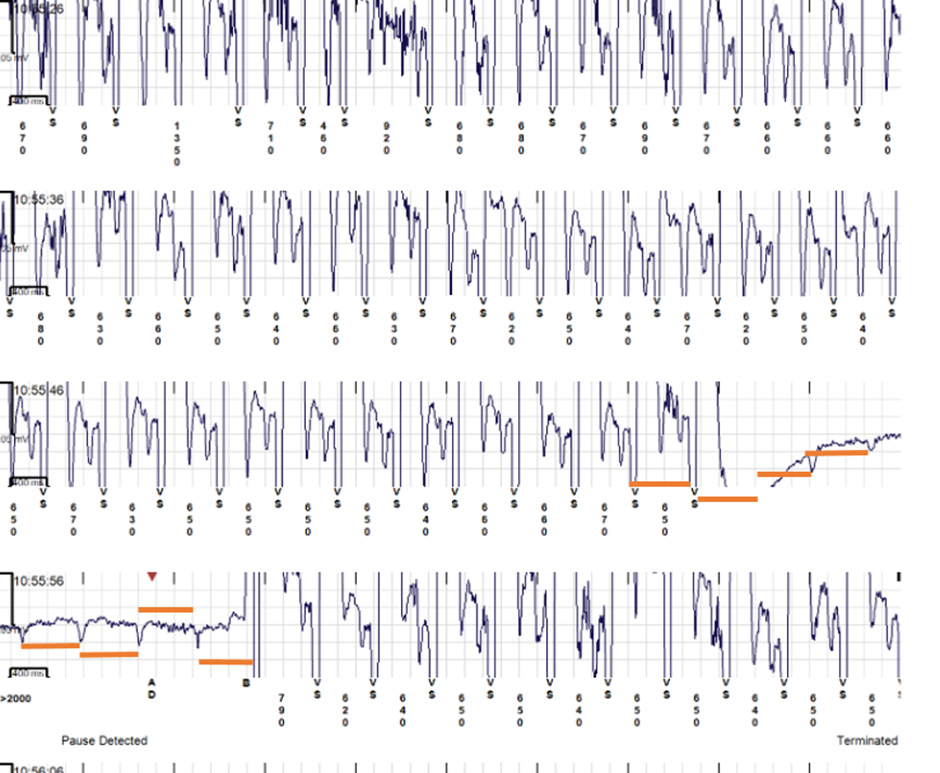
Figure 1
Discussion
Implantable Loop Recorder’s (ILR) provide an extremely useful diagnostic tool for patients with suspected arrhythmia, particularly among those who experience infrequent episodes of syncope (Choi, et al, 2022).
With the emergence of remote monitoring the amount of data being received from these devices is great and therefore particular care is necessary when analysing said data to ensure that the correct treatment steps are initiated and followed, if required at all.
On Figure 1 we can see the transmitted episode from the ILR to the remote monitoring website. It appears to show normal sinus rhythm followed by an episode high grade AV Block before resumption of normal sinus rhythm.
Figure 2 shows that by increasing the gain of the transmitted episode we can clearly see the presence of the undersensed QRS complex being conducted in 1:1 pattern. Additionally, note the regular R-R interval showing clearly that this is not high grade AV Block.
An explanation from the manufacturer was sought which was as follows:
“A temporary gain may occur if the device loses contact with the skin, as seen in this example. This has been resolved by the end of the strip.
There is no indication of device issue or concern, this is most likely related to a physiological origin.”
O’ Shea et al, (2021) in a study of 1470 patients found that 2292 (76.8%) asystole alerts were false positive and 192 episodes (27.8%) were false- positive for bradycardia. They found that all false positive for asystole and bradycardia were for undersensing. ILR alerts require careful assessment given that more than half may not reflect a true arrhythmia; assessment by qualified cardiac device specialists can lessen the proportion of alerts that are unnecessarily escalated to the treating clinician.
As in this example great care is needed to ensure that patient’s do not receive pacemakers that are not indicated.
References
- Choi, Y.Y., Choi, JI., Kim, Y.G. et al. Diagnostic usefulness of implantable loop recorder in patients with unexplained syncope or palpitation. Int J Arrhythm 23, 17 (2022). https://doi.org/10.1186/s42444-022-00068-w
- O’Shea, C., Middeldorp, M., Hendriks, J. et al. Remote Monitoring of Implantable Loop Recorders: False- Positive Alert Episode Burden. Circulation: Arrhythmia and Electrophysiology 14, 11, (2021), https://www.ahajournals.org/doi/full/10.1161/CIRCEP.121.009635
Disclaimer: The British Heart Rhythm Society (BHRS) collates submissions for the ECG/EGM challenge on this website. These submissions, along with any accompanying answers, are provided by external contributors and are published for informational purposes only. BHRS does not endorse, guarantee, or warrant the accuracy, completeness, or reliability of any submissions or answers provided.