

December 2023
A case of inter-pacemaker crosstalk
Daniel Hunnybun Highly Specialised Cardiac Physiologist, Northern General, Sheffield, UK
Disclosure: The author has no conflict of interests to declare.
Background
A patient with adult congenital heart disease presented to pacing clinic with palpitations. Notably the patient had 2 pacemakers in situ.
The patient had a epicardial dual chamber ELA medical pacemaker implanted following their TCPC surgery in 2004 due to sinus arrest. In 2022 the patient had an endocardial single chamber atrial Medtronic device implanted following RV lead failure and the inability to programme around far field R wave oversensing. Following the transvenous device implant the epicardial and endocardial devices were programmed to AAI 30bpm and AAIR 70bpm respectively.
On presentation in pacing clinic the following EGMs/ECGs were recorded (Figure 1.).
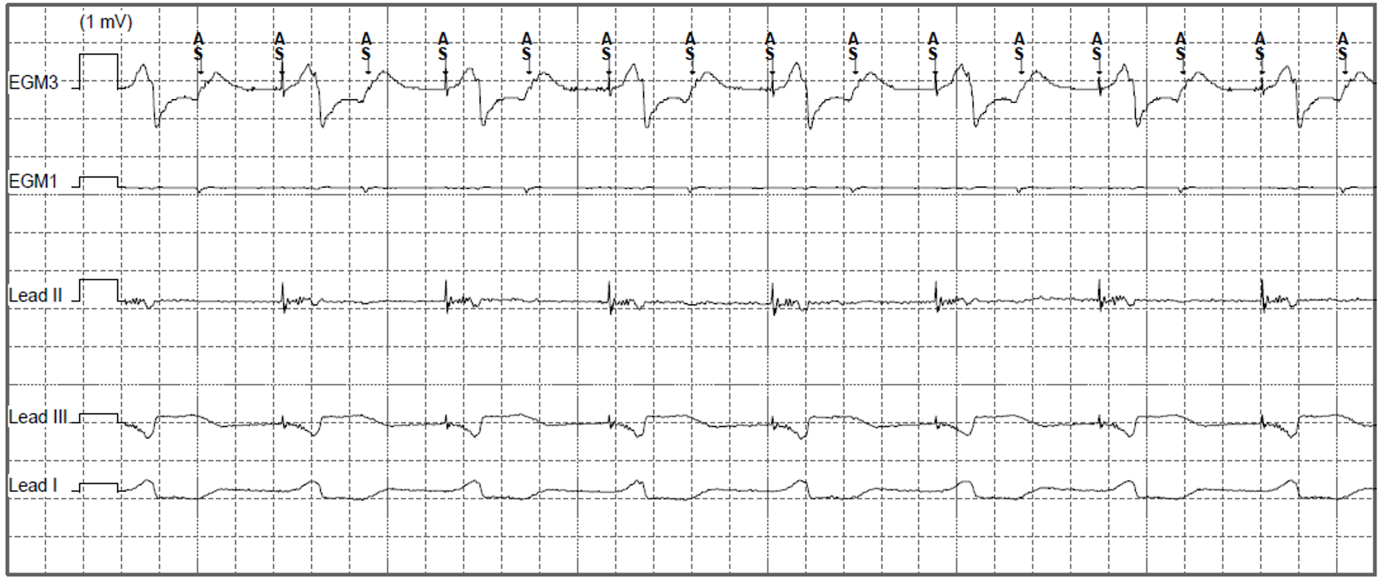
Figure 1. Presenting EGM in pacing clinic (EGM3: Can-Aring, EGM1: Atip-Aring).
The epicardial device was found to be at ERI and had consequently mode switched to VVI 70bpm with unipolar pacing (5V@1ms). As well as VA conduction, inter-pacemaker crosstalk can explain the higher sensed atrial rate seen in Figure 1 (Bardia et al. 2022). The epicardial device was reprogrammed to VVI 30bpm with cessation of ventricular pacing. The patient was then admitted for their epicardial device to be explanted.
The following morning the patient’s symptoms returned with the telemetry changes seen in Figure 2.

Figure 2. Telemetry changes at time of symptom onset.
QUESTION
What is the most appropriate programming change to resolve the patient’s ongoing symptoms?
Answer
Increase the lower rate of the endocardial atrial device
Explanation/Discussion
The telemetry changes seen are most likely caused by ventricular under sensing by the epicardial device. As a result of inter-pacemaker crosstalk, the endocardial atrial timing cycle was reset, thereby delaying the next atrial stimulus. This delay was sufficient to permit ventricular pacing from the epicardial device prior to AV conduction. As both devices were programmed to 70bpm, the patient was then locked into this atrial paced, ventricular paced rhythm with an apparent short atrioventricular delay.
Reducing the lower rate limit or reprogramming the epicardial device to ODO would only prevent back up mode until the next battery test. Increasing the sensitivity of the epicardial device is a reasonable strategy, however given known issues with the RV lead, this may not prevent future oversensing (Figure 3).


Figure 3. Telemetry changes with timing cycles superimposed. Following ventricular under sensing and inter-pacemaker crosstalk (*) the patient was locked into atrial pace, ventricular pace with an apparent short atrioventricular delay (Orange: Epicardial ventricular lower rate timing cycle, Blue: Endocardial atrial lower rate timing cycle).
Increasing the endocardial atrial pacing rate would prevent (or at least shorten) these episodes. A shorter atrial pacing cycle length would result in earlier atrial pacing and subsequent AV conduction, allowing for another opportunity for adequate ventricular sensing. Even if this doesn’t avoid ventricular pacing, the high atrial pacing rate would promote ventricular conduction and prevent ongoing inappropriate ventricular pacing.
Following the increase of the endocardial atrial pacing rate to 80bpm, ventricular pacing ceased, and the patient’s symptoms resolved (Figure 4). Interestingly, immediately following programming the next ventricular rate exceeds that of programmed VVI back up mode. Therefore, in this case, there must have also been inter-pacemaker crosstalk from endocardial atrial pacing. However, as both devices were programmed to 70bpm, both devices were pacing almost simultaneously preventing such inter-pacemaker crosstalk during symptomatic episodes.
The patient had their epicardial device explanted and was discharged a few days later without complication. Being aware of inter-device interactions, such as these, is important to avoid comprising patient morbidity, particularly for those at risk of heart failure decompensations (Bardia et al. 2022).
Figure 4. Telemetry changes seen following reprogramming of the endocardial atrial device.
References
Bardia et al. 2022. Inter-pacemaker crosstalk – A cause for CRT failure. JACC, 79 (9). Doi: https://doi.org/10.1016/S0735-1097(22)03429-5open_in_new
Disclaimer: The British Heart Rhythm Society (BHRS) collates submissions for the ECG/EGM challenge on this website. These submissions, along with any accompanying answers, are provided by external contributors and are published for informational purposes only. BHRS does not endorse, guarantee, or warrant the accuracy, completeness, or reliability of any submissions or answers provided.