

February 2024
Change in pacing thresholds causing bradycardia – but what algorithm facilitates this?
Adam Marzetti Invasive Lead Cardiac Physiologist, East Kent Hospital University Foundation Trust, UK
Disclosure: The author has no conflict of interests to declare.
Background
A 73 year old lady with a history of paroxysmal atrial fibrillation (PAF) and sinus node dysfunction, had a dual chamber pacemaker implanted in 2018. In July 2023, she was prescribed Flecainide for ongoing PAF.
In December 2023 she presented to the emergency department with fast AF, and was given intravenous amiodarone. After the rhythm was terminated, she became bradycardic at 40bpm in a junctional escape rhythm (see figure 1).
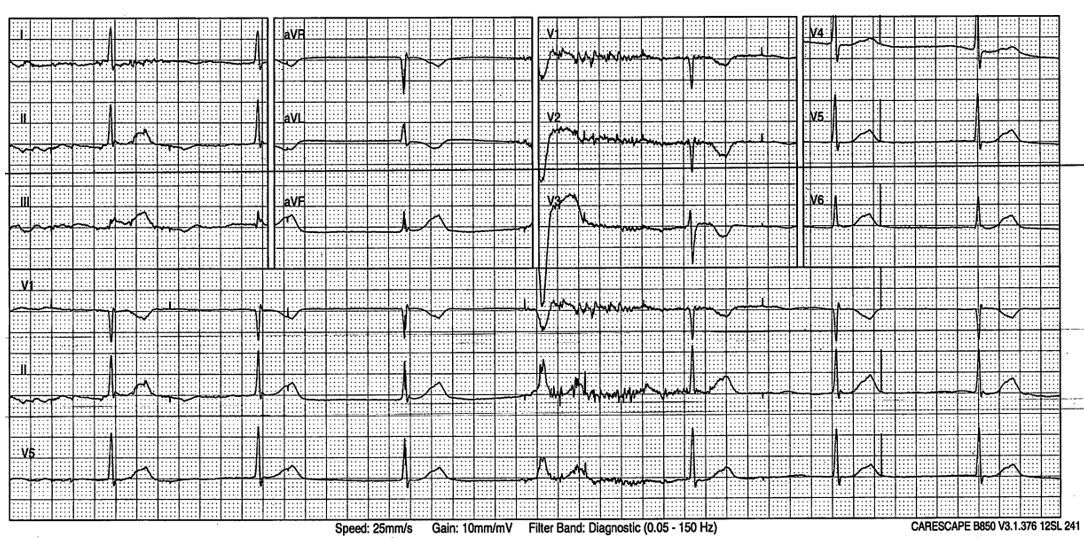
QUESTION
The ECG shows loss of atrial capture, but the question of the physician was why is the device not pacing in the ventricle? What mode is this?
Answer
AAIR<>DDDR (MVP)
Explanation/Discussion
The device is a Medtronic Ensura programmed AAI<>DDD (first generation). When MVP is functioning on AAIR mode, as in this case, ventricular backup pacing occurs following 2 out of 4 A-A intervals that do not have a ventricular sensed event. The device then back-up paces 80ms after the A-A escape interval(1). When applied to this ECG, the first two atrial pacing spikes with loss of A-Capture, only one has a valid V-Sense event. The third escape beat of the ECG coincides with the atrial pacing spike and so does not have a valid V-sense event. As now 2 out of four A-A intervals do not have ventricular sense events, the device delivers back-up ventricular pacing 80ms after the atrial paced event. Because this is a temporary switch, the device does not continue to deliver ventricular pacing as some of the junctional escape beats, fall into the V-Sense event window, preventing the switch to DDD mode. Figure 2 demonstrates the annotated ECG, the green VS markers highlight valid V-Sensed event after an atrial pacing event, the red VS markers are invalid V-Sensed events.
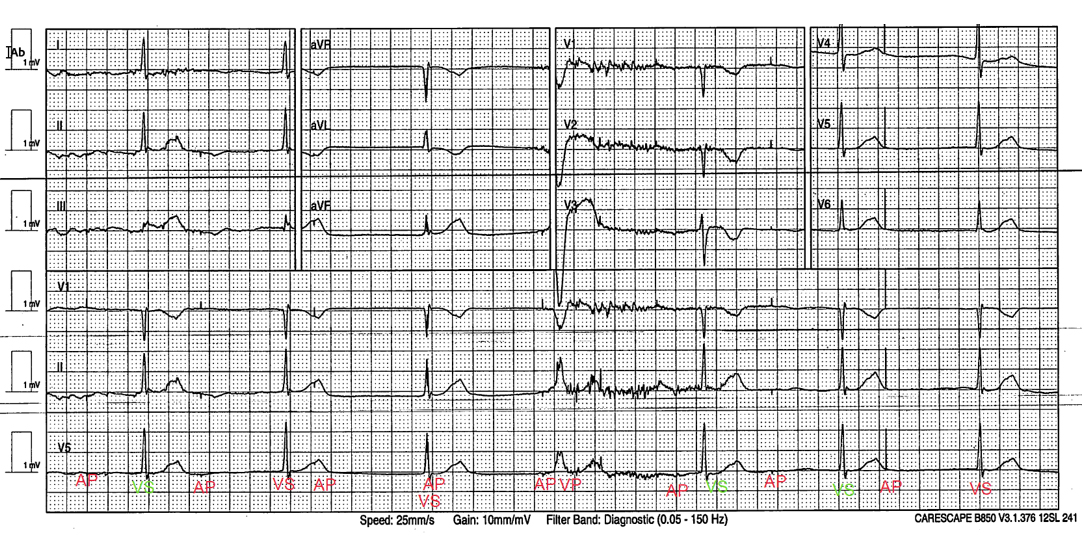
Figure 2: Annotated 12-Lead ECG
Interestingly, the patient had been started on Flecainide in July 2023 for her PAF. Figure 3 below shows the atrial capture management trend, demonstrating the atrial threshold had begun to rise almost immediately after commencing treatment.

Figure 3: Atrial Capture Management Trend
Flecainide can be associated with a rise in pacing thresholds and intermittent loss of capture(2) is reported in the literature. This is because as a class IC agent, flecainide markedly depresses rate of rise in the cardiac action potential, but a relatively small effect on the action potential duration(3). In this case, the device was reprogrammed to DDDR with a long AV delay, with the atrial outputs being increased to restore atrial capture and AV synchrony. The purpose of this is to provide atrial pacing as required by this patient, and to still allow intrinsic conduction and reduce unnecessary right ventricular pacing. The presence of an active AV delay in DDDR mode will ensure that any atrial paced event will always result in a ventricular paced event, should atrial loss of capture recur.
References
1. Medtronic Academy. (2023). Managed Ventricular Pacing (MVP) Features. Available at: Managed Ventricular Pacing (MVP) Features (medtronicacademy.com)
2. Suffrendi, J. Rutland, J. Akpunonu, P. Baum, R. Catanzaro, J and Elayi, C. (2019). ‘Flecainide Toxicity Resulting in Pacemaker Latency and Intermittent Failure to Capture.’ American Journal of Case Reports. Volume 20. DOI: https://doi.org/10.12659%2FAJCR.916370
3. Hellestrand, K. Nathan, A. Bexton, R. Camm, A. (1984). ‘Electrophysiologic effects of flecainide acetate on sinus node dysfunction, anomalous atrioventricular connections, and pacemaker thresholds’. American Journal of Cardiology. 53(5). 30B-38B. DOI: 10.1016/0002-9149(84)90499-5
Disclaimer: The British Heart Rhythm Society (BHRS) collates submissions for the ECG/EGM challenge on this website. These submissions, along with any accompanying answers, are provided by external contributors and are published for informational purposes only. BHRS does not endorse, guarantee, or warrant the accuracy, completeness, or reliability of any submissions or answers provided.