

February 2020
Ventricular Ectopy: Site of Origin
Dr Heather Edwards
ST5 Cardiology SpR at University Hospital Wales
mailto:h.edwards24@googlemail.com

Figure 1
12 lead ECG with ventricular ectopy
QUESTION
Where is the origin of the PVC’s?
Answer
RVOT
Discussion
If the PVC is originating from the RVOT it is likely to have a LBBB pattern and an inferior axis (positive QRS in inferior leads). There may be a small R waves present in V1 if the origin of the ectopic is from the posterior RVOT. There will also be small R waves present in the left and Right coronary cusps. The R waves in the left coronary cusp is smaller than one would assume as there is very little myocardium adjacent to this structure to generate a large R wave. Complexes originating from the aortomitral continuity have a dominant R wave in V1 and RBBB pattern.(1) If the precordial transition is later than in sinus rhythm The PVC is likely to be RVOT. If the pre cordial transition earlier than in sinus rhythm then likely to be LVOT(2)
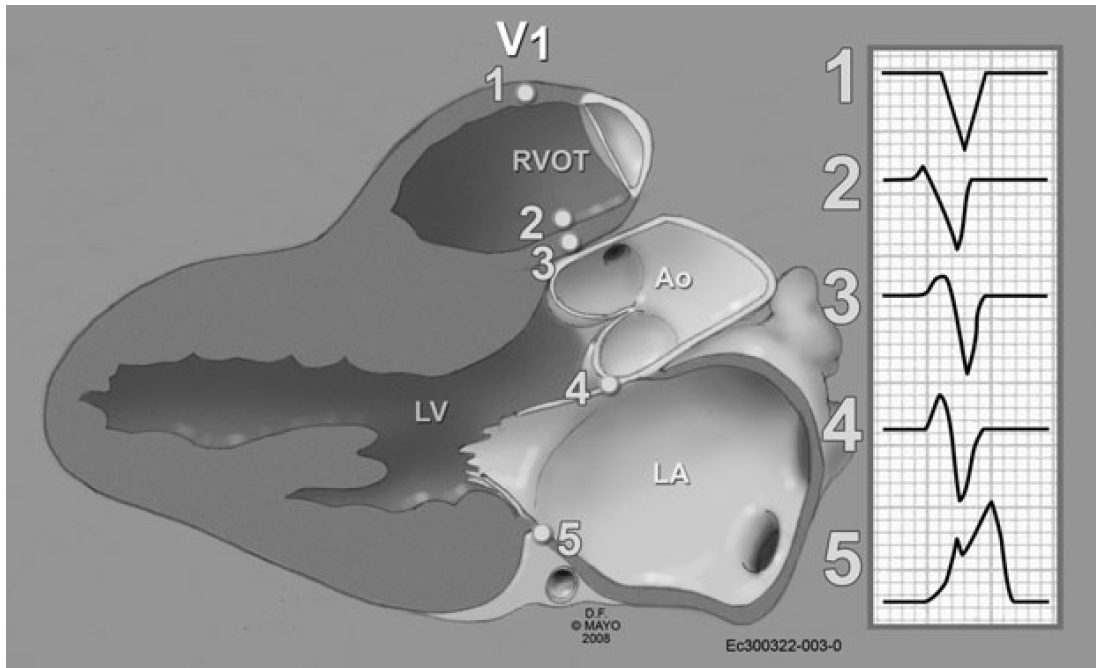
1. Anterior RVOT
2. Posterior RVOT
3. Anterior RCC
4. Posterior LCC
5. Aortamitral continuity
Figure 2
Correlative Anatomy for the Invasive Electrophysiologist:Outflow Tract and Supravalvar Arrhythmia J Cardiovasc Electrophysiol, Vol. 20, pp. 955-968, August 2009 (3)
References
1. Supravalvular Arrhythmia. Identifying and Ablating the Substrate. Niloufar Tabatabaei, Samuel J. Asirvatham. Circ Arrhythm Electrophysiol. 2009;2:316-326.
2. The V2 Transition Ratio: A New Electrocardiographic Criterion for Distinguishing Left From Right Ventricular Outflow Tract Tachycardia Origin. Brian P Betensky et al. JACC Vol. 57 issue 22 31.5.2011 P 2255 – 2262
3. Correlative Anatomy for the Invasive Electrophysiologist:Outflow Tract and Supravalvar Arrhythmia J Cardiovasc Electrophysiology. Samuel J. Asirvatham. Vol. 20, pp. 955-968, August 2009