

June 2018
What is the cause of this Mode Switch Episode?
Holly Daw – Chief Cardiac Physiologist
Barts Heart Centre, West Smithfield, London EC1A 7BE
holly.daw@bartshealth.nhs.uk
Background
A 56 year old male with a history of paroxysmal atrial fibrillation (AF) with poor rate control during AF episodes, sick sinus syndrome and an ejection fraction < 45%, was considered for an AV node ablation, with intention to implant a cardiac resynchronisation therapy pacemaker (CRT-P). Initial implantation was in 2014, where a Biotronik Evia HF-T pulse generator was implanted. Active fixation leads were positioned to the right atrial appendage and right ventricular apical septum. An attempt at left ventricular (LV) lead placement was unsuccessful and the LV port was plugged. Following implant and without undergoing an AV node ablation there was improvement in symptoms. The decision was made not to re-attempt LV lead implantation with the device programmed to function as a dual chamber pacemaker. Since implant there has been normal pacing function. The RA threshold which was accepted as high during implant has remained high but stable. All other lead measurements have been within normal limits. Episodes of mode switch have been seen on device interrogation as expected with a history of PAF. However, one interesting EGM recorded as a mode switch episode is displayed below.
Mode: DDD
LRL / MSR: 50 / 120
AVD: Dynamic 150 / 120
RA output: 2.5V @ 1.0ms
RV output: 1.5V @ 0.4ms
IRS Plus and Capture Control On
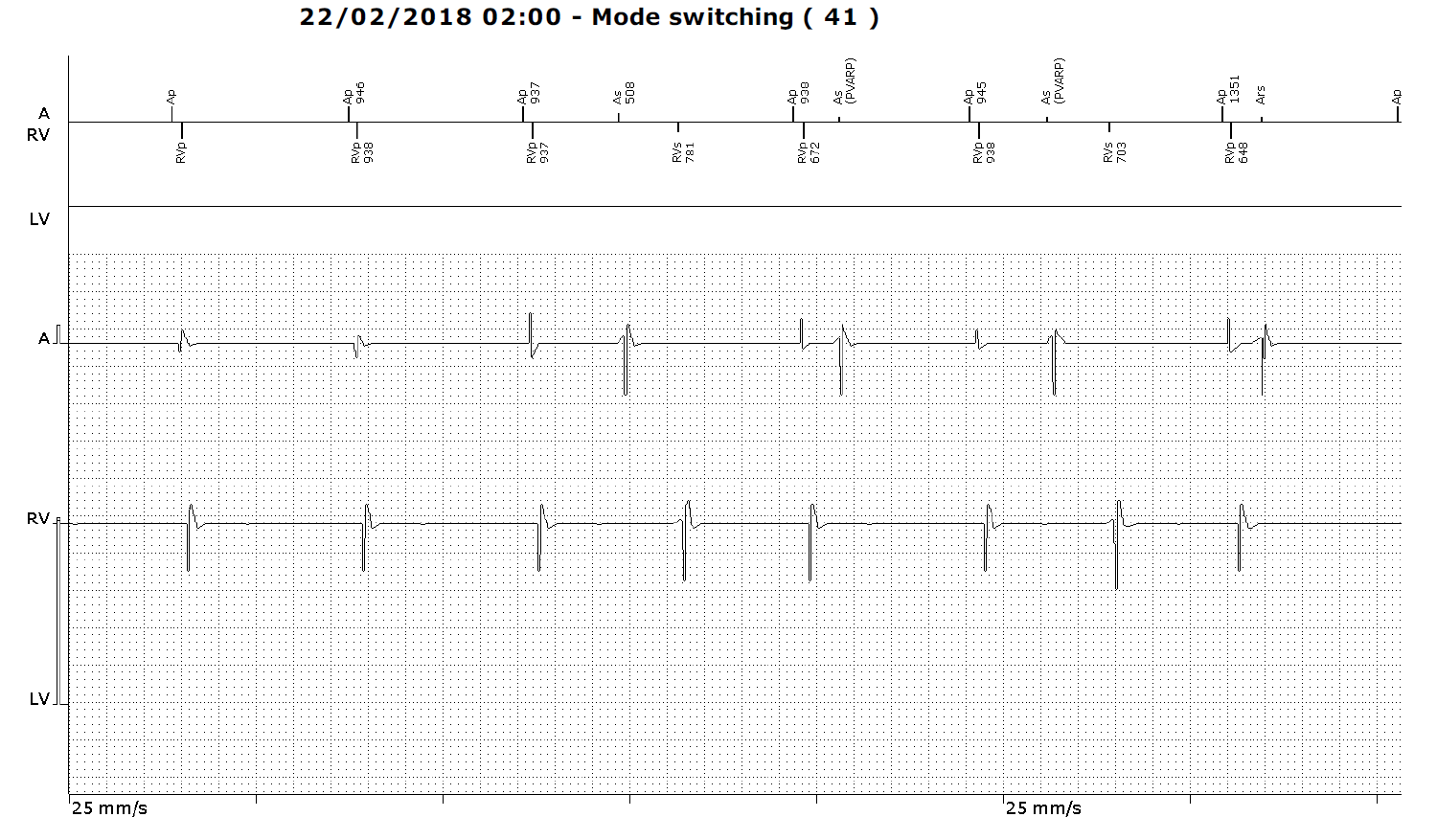

Figure 1
Stored electrogram. Top to bottom, marker channel, LV marker channel (plugged), atrial electrogram, ventricular electrogram.