

March 2019
An unscheduled remote transmission received for ‘shock delivered’




THE QUESTION
What is the cause of the shock received by the patient?
Answer
RV lead oversensing atrial fibrillation causing an inappropriate schock
Explanation
In this case the R wave measurement, presenting EGM and far field EGM displayed in the shock episode help determine the cause of this patient’s shock therapy.
- The measured R wave of 1.3 mV is very low for a typical R wave expected in an ICD system. This raises suspicion that there may be a problem with R wave sensing and that there may be an issue with the lead position.
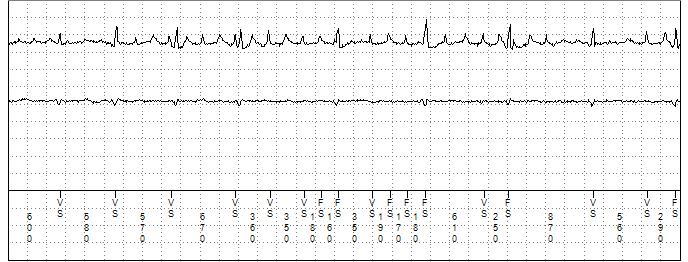
- The presenting EGM in figure 1 shows a near field EGM which has atrial and ventricular signals present. The EGM is displaying oversensing of atrial fibrillation by the ventricular lead in addition to appropriately sensed R waves, with sensed events marked as ventricular sense (VS) and ventricular sense in the VF zone (FS). The latter would count towards tachyarrhythmia detection criteria.
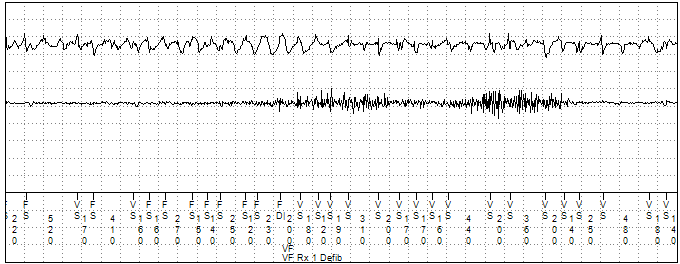
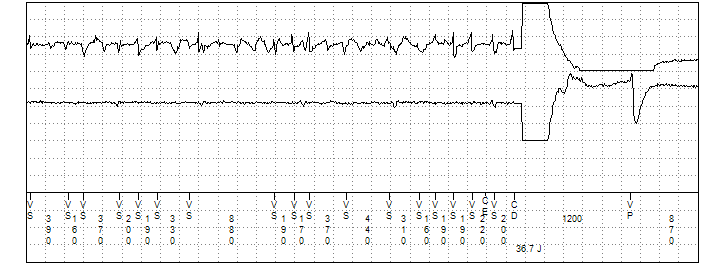
- The shock episode displays near field and far field EGM’s which do not match, best seen in the strip in figure 3. At first glance the near field EGM looks consistent with an episode of ventricular fibrillation (VF). However, the far field EGM a ‘unipolar’ channel which resembles a surface ECG, displays low amplitude R waves at irregular intervals consistent with an underlying rhythm of permanent atrial fibrillation. If the episode was a true VF or polymorphic ventricular tachycardia (PMVT) the near and far field EGM’s would be expected to be similar in appearance.
- Other possibilities of RV lead fracture or EMI causing the shock can also be ruled out as the EGM does not display make break type signals associated with a lead fracture or high frequency electrical signals on both near and far field EGM’s which would be characteristic of EMI. There are high frequency signals seen on the far field EGM at the start of the shock recording where there is a section of artefact however these are caused by the ‘unipolar’ EGM detecting pectoral myopotentials and do not count towards sensing or detection criteria.
Patient Management
The patient was told to attend his local A&E where his ICD was interrogated. The device check confirmed poor R wave sensing with an R wave of 1.3 mV previous recorded at 12mV. The RV lead was also found to not capture the ventricle even at high outputs. RV lead displacement was suspected and a chest X ray was performed, shown in figure 4. The PA chest X-ray confirmed that the RV lead had displaced and was sitting at the Tricuspid valve level which explains why atrial and ventricular signals had been present on the initial remote transmission EGM.
.png)
Figure 4
PA chest X-ray performed in A&E clearly showing the ventricular lead to have displaced which was sitting at the Tricuspid valve level
The ICD was deactivated in A&E to prevent any further inappropriate therapies, the patient placed on monitoring and admitted for further management. The next day the patient was taken to the catheter lab where the displaced lead was removed and a new RV single coil active fix ICD lead positioned to RV apex. Satisfactory checks and position were obtained peri-operatively and post-operatively. The patient was discharged and has had no further complications to date.