Answer
The answer is surgical procedure
Explanation
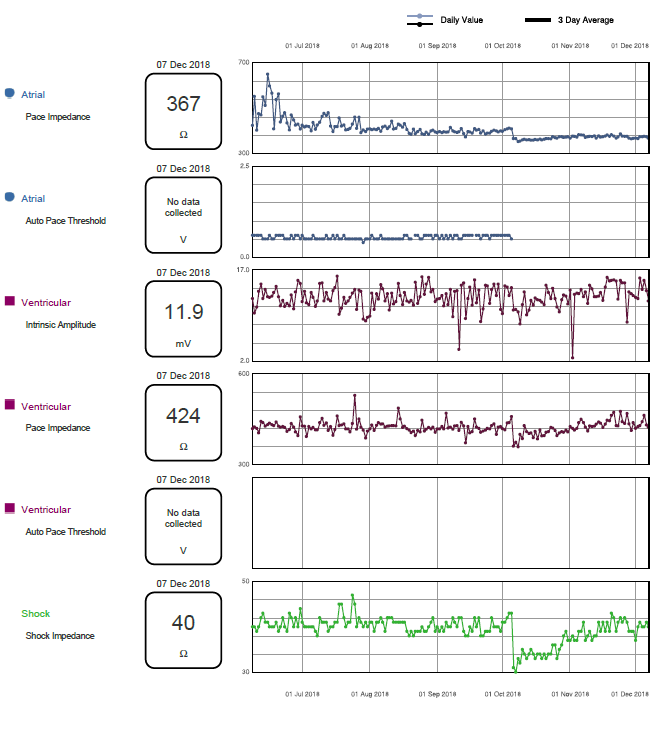
The patient underwent aortic root and valve replacement in October 2018. At this time a significant change in lead and diagnostic trends is observed.
- Atrial lead bipolar impedance drops suddenly as does intrinsic P wave size; this can be explained by a subtle change in lead positioning and / or right atrial (RA) characteristics following surgical intervention (such as atriotomy cannulation for cardio-pulmonary bypass). Although RA impedance then stabilises at new levels, intrinsic P wave amplitude appears to gradually improve, suggestive of improving or recovering RA myocardial activity.
- Right ventricle (RV) lead bipolar pacing impedance and shock vector impedance both drop suddenly at time of surgery before gradually returning to pre-procedure levels. This is most likely due to localised oedema following surgery, which is why the relatively small bipolar pace circuit is less affected and returns to baseline sooner than the larger vector of RV coil to can which includes myocardium, lung tissue, chest wall and pectoral muscle.
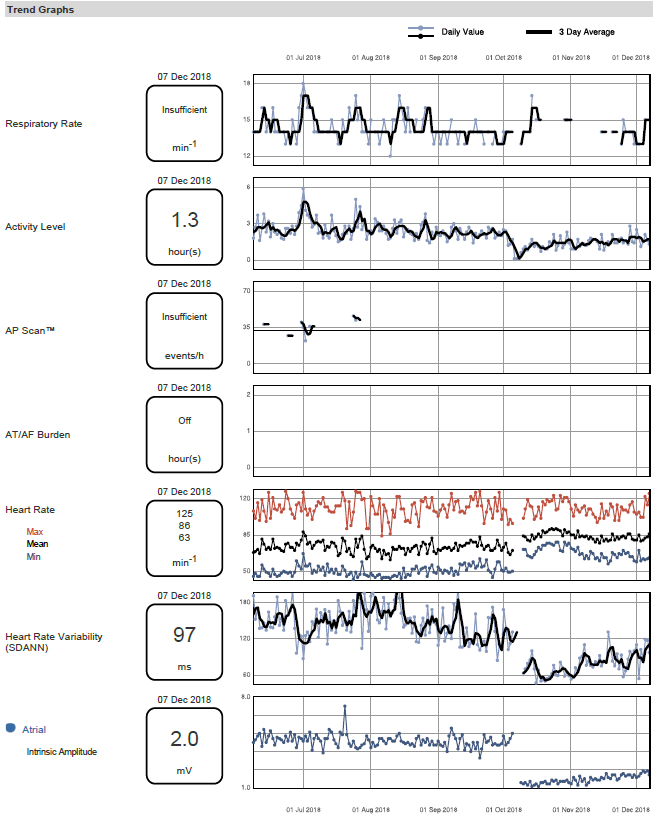
- Diagnostic trends show a sudden reduction in patient activity level that persists for several weeks. Although maximum heart rate (HR) is not affected both minimum HR and average HR increase post-surgery with a corresponding drop in HR variability (SDANN – Standard Deviation Average Normal to Normal). Both trend graphs are beginning to return to pre-surgical levels by the time of this download.
All lead measurements remain within normal limits throughout but demonstrate sudden changes occurring at the time of surgical intervention. That these changes are present in both RA and RV leads and across a number of measured parameters is highly suggestive of an external event rather than ICD generator or lead failure. The changes in the patient’s clinical status (HR, HR variability, activity levels) further supports an external event occurring. If this event was merely a change in medical regime no gradual return to baseline levels would be expected, or change in patients clinical status.