

ECG/EGM Challenge Answer:
Minute ventilation sensor
Sam Griffiths – Senior Cardiac Physiologist
s.griffiths4@rbht.nhs.uk
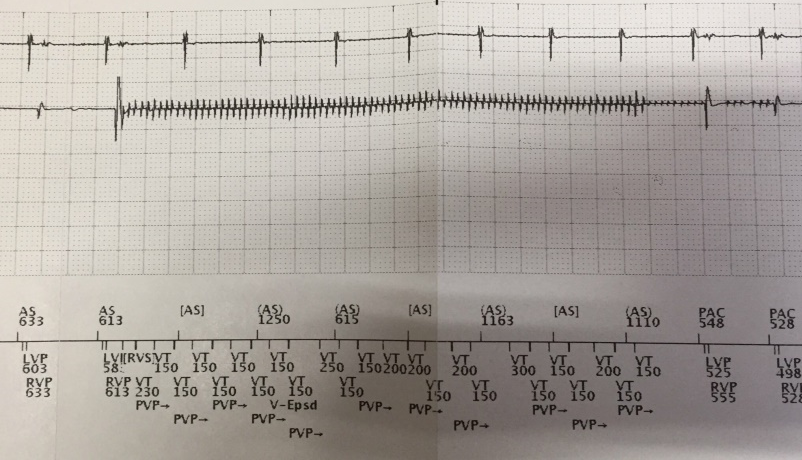

Figure 1
Stored EGM strip of a ventricular high rate episode. Top to bottom: Atrial EGM (5 mm/mV), right ventricular EGM (1 mm/mV), marker channel.
Answer
Minute ventilation sensor
Explanation
The EGM displayed in figure 1 is an example of pacing inhibition due to oversensing of the minute ventilation sensor signal. The EGM starts with two tracked sinus p waves at a rate of approximately 100 bpm followed by biventricular pacing (AS/BiVP). There is then a sudden onset of high frequency signals on the ventricular EGM that are sensed by the device at 150, 200 and 300ms intervals. Ventricular oversensing of the high frequency signals results in ventricular pacing inhibition which essentially causes a 4.5 second episode of ventricular standstill resulting in a pre-syncopal episode.
On closer inspection, the signals on the ventricular channel occur in 50ms intervals. They are clearly too fast to be physiological ruling out ventricular tachycardia. The signals are only present on the RV electrogram which would tend to rule out an external source of EMI which is more typically seen on both the atrial and ventricular channels. The signals are not consistent with those seen with a lead fracture which tend to be more erratic and of higher amplitude than the signals in this episode. They also do not look typical of myopotential signals which would be expected to be displayed with high frequency but with a ‘crescendo-decrescendo’ appearance.
In cases where there is a lead integrity issue that creates high impedance states, minute ventilation signals can be sensed by some pacemakers. A recent field safety notice and medical device alert explaining this malfunction and advice on action to take is available here.